
#1. Migraine researchers at Yale don’t use microdoses in their studies.
Evidence seems to suggest that a microdose for migraines is just not enough. In the Yale Medicine clinical trials for psilocybin and migraine disease, the doctors overseeing the studies opt not to utilize microdosing as a treatment approach for migraines. For those grappling with migraines, a less frequent dosing schedule with slightly higher doses may offer a more promising alternative to the conventional microdosing protocol, which involves administering numerous small doses per week.
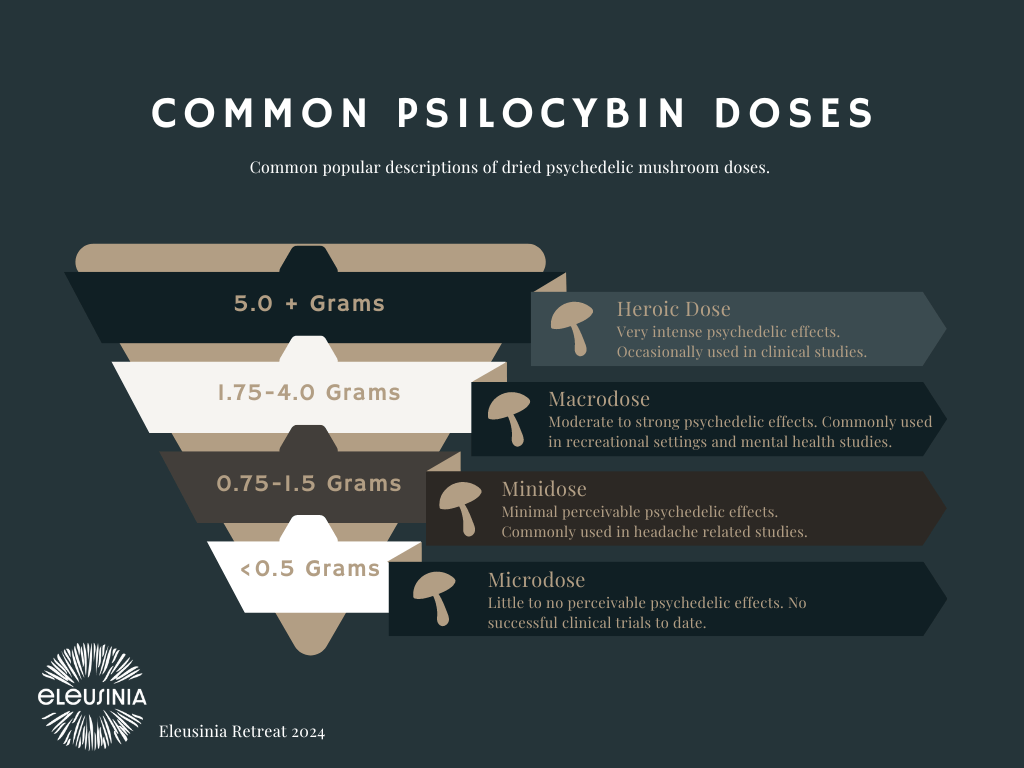
In these clinical trials, doses equivalent to 1.0 to 1.5 grams of dried mushrooms are administered every two weeks for migraine treatment. These doses typically result in effects akin to consuming an alcoholic beverage or using cannabis products, thus unlikely to induce an intense experience. However, it’s crucial to acknowledge that individual tolerance levels and experiences may vary.
Refer to the chart below for a breakdown of the doses and their common terminology.
#2 Watch out for the rebound.
The consumption of psilocybin mushrooms can potentially trigger a rebound headache in some individuals. Microdosing for migraine may result is initially experiencing a headache before seeing improvement. While the severity of these rebound headaches can vary, experiencing them following dosing may still lead to an overall reduction in headaches. It’s important to prepare yourself for potential rebound headaches.
#3. Get a good scale.
Having a sensitive scale is crucial for accurate measurement. To ensure you find one that meets your needs, consider searching for a “jeweler’s scale.” These scales are typically sensitive enough to measure in milligrams, making them suitable for your requirements. It’s worth noting that most standard food scales may not offer the necessary sensitivity to measure fractions of a gram, hence investing in a specialty scale is necessary.

Microdosing mushrooms for migraine requires precision.
#4. Stay consistent.
Microdosing for migraines works best with consistency. Specifically by growing your own supply, you guarantee that you will have no interruptions in treatment. There are various videos online explaining the cultivation process, including the series created by Eleusinia Retreat. If you attend one of our retreats, there is a comprehensive mushroom growing course.
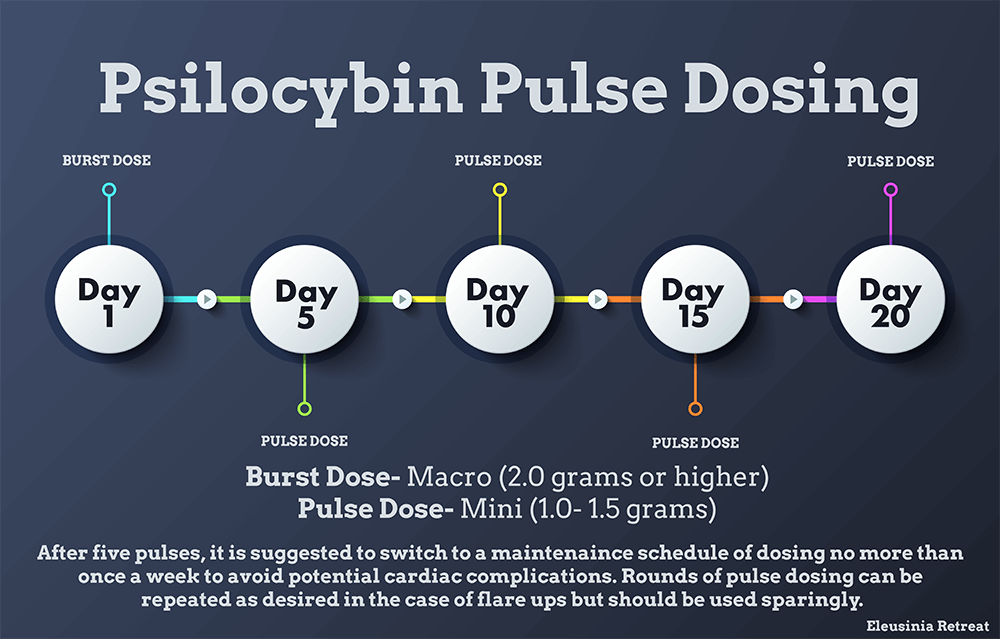
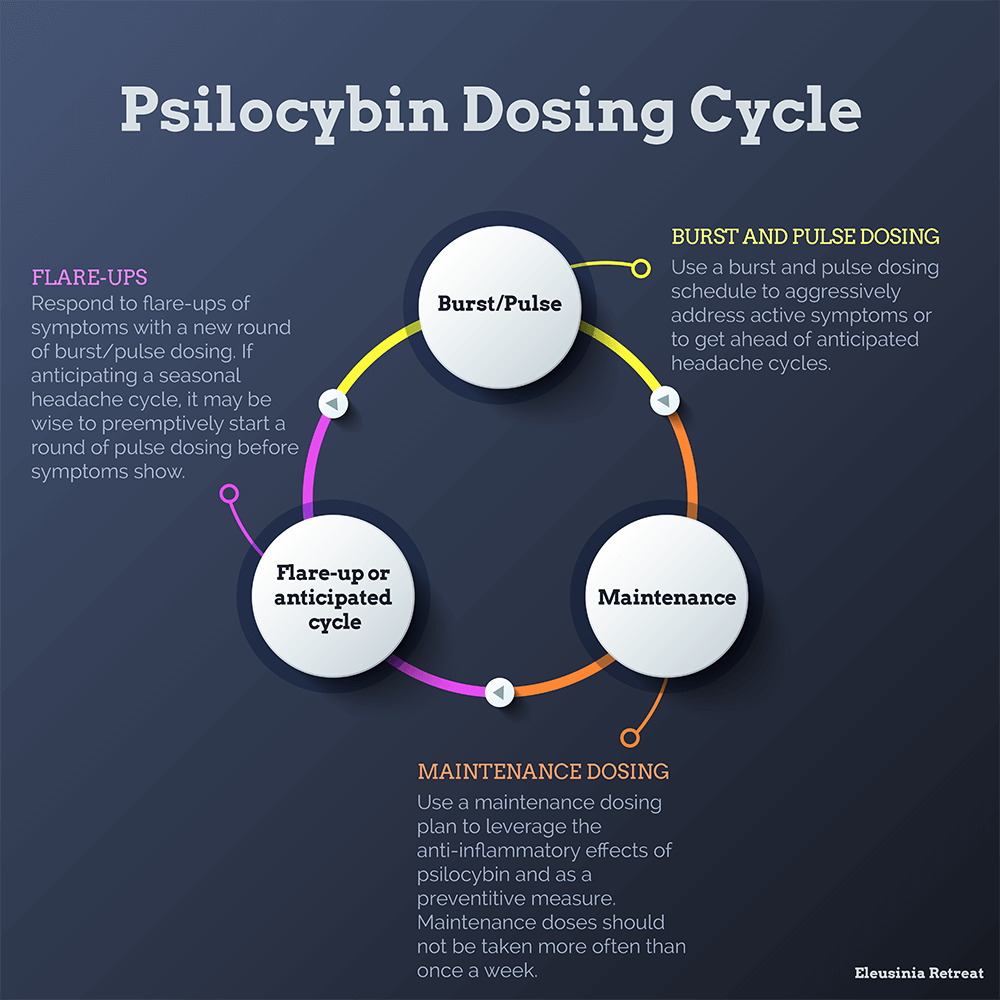
The chart below describes how to use doses slightly larger than the typical microdose to manage migraine.
#5. Consider DMT as an alternative.
At Eleusinia Retreat, we’ve observed that visitors often find more success in managing migraines with DMT compared to psilocybin. Microdosing psilocybin for migraines lacks robust clinical evidence supporting its efficacy, and many individuals either don’t experience significant results or find them to be short-lived.
DMT is recognized by numerous cluster headache and migraine sufferers as both an abortive and a preventative measure. It’s highly effective at halting a migraine attack and requires significantly less time than a psilocybin minidose, with effects lasting typically 5-10 minutes when taken in small doses.
Our program at Eleusinia Retreat not only provides psilocybin and DMT experiences but also includes classes on cultivation and extraction. This empowers visitors to independently manage their migraines beyond the retreat setting.





3 Responses
Thank you for writing this guide, most sites discuss microdosing in relation to migraines but I’ve found bigger, less frequent doses to be more effective. I’m interested in trying this schedule next time I flare up.
One quest: Is a maintenance dose the same amount as a pulse dose?
I had the same question about the maintenance dose. Assuming it’s somewhere around 1g or less, but would be nice to know for sure.
I tried 999 mg. The nausea was unreal (even used zofran) and I tripped hard for 6 hours. I cannot imagine doing this every 2 weeks. Micro dosing will have to do for me.